
Dental Prophylaxis Risk Assessment Tool
Risk Assessment Results
Low Risk Factors
Minimal health concerns and gentle prophylaxis methods.
MinimalModerate Risk Factors
Some health issues or moderate prophylaxis methods used.
ModerateHigh Risk Factors
Multiple health concerns or aggressive prophylaxis methods.
HighLesion Types to Watch For
- Aphthous ulcers
- Candidiasis
- Mucositis
- Hyperkeratotic patches
Key Takeaways
- Prophylactic dental care can both prevent and, in rare cases, trigger oral lesions.
- Mechanical cleaning, chemical rinses, and fluoride applications have distinct risk profiles.
- Patients with compromised immunity, xerostomia, or chronic disease need tailored prophylaxis.
- Choosing the right adjuncts (e.g., chlorhexidine vs. essential oil mouthwash) can reduce lesion incidence.
- Regular monitoring and prompt lesion assessment are essential for safe preventive care.
When we talk about Prophylaxis the preventive care practices aimed at maintaining oral health and preventing disease, the image that comes to mind is a sparkling smile after a routine cleaning. Yet, the same preventive steps can sometimes set the stage for unwanted tissue changes in the mouth. Understanding the link between prophylactic interventions and the development of oral lesions helps clinicians balance protection with potential side‑effects.
What Is Dental Prophylaxis?
In dentistry, prophylaxis covers a spectrum of actions that keep the oral environment clean and disease‑free. These actions fall into three major groups:
- Mechanical cleaning - scaling, polishing, and ultrasonic debridement performed by a dental hygienist.
- Chemical adjuncts - antimicrobial mouthwashes, such as chlorhexidine, and topical agents like povidone‑iodine.
- Fluoride therapies - varnishes, gels, or rinses that strengthen enamel.
Each group targets the primary culprit of dental disease: dental plaque a biofilm of bacteria that adheres to tooth surfaces. By disrupting plaque formation, prophylaxis reduces caries and periodontal disease, the two most common drivers of oral pathology.
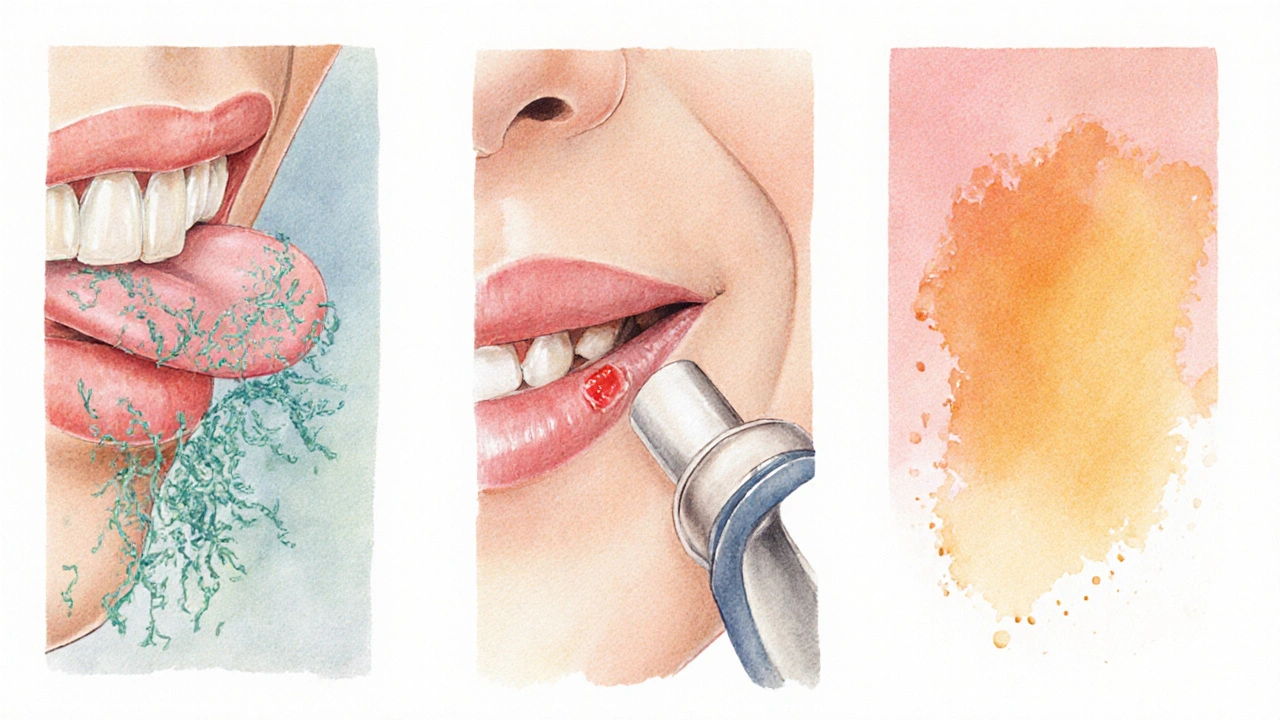
Defining Oral Lesions
Oral lesions any abnormal change in the mucosal tissue of the mouth, ranging from harmless ulcers to precancerous growths encompass a wide variety of conditions. The most frequently encountered types include:
- Aphthous ulcers - small, painful sores often linked to stress or nutrient deficiency.
- Candidiasis - fungal overgrowth, especially in patients with dry mouth or immunosuppression.
- Mucositis - inflammation caused by chemotherapy, radiation, or harsh oral care products.
- Hyperkeratotic lesions - thickened patches that may arise from chronic irritation.
- Oral squamous cell carcinoma - malignant growths that can be missed if routine examinations are lax.
While many lesions are benign and self‑limiting, early detection is crucial because some can signal systemic disease or progress to malignancy.
How Prophylaxis Influences Lesion Development
Prophylactic measures are generally protective, but several mechanisms can inadvertently foster lesion formation:
1. Disruption of the Natural Microbiome
Chemical rinses, especially broad‑spectrum agents like chlorhexidine, dramatically lower bacterial counts. While this curtails plaque, it also reduces commensal species that compete with opportunistic fungi. In patients with reduced salivary flow, this imbalance can encourage candidiasis a yeast infection caused by Candida species on the tongue, palate, or denture surfaces.
2. Physical Irritation from Mechanical Tools
Ultra‑high‑speed scalers generate heat and micro‑trauma. For patients with fragile mucosa-such as those on bisphosphonates or with autoimmune diseases-repeated scaling can precipitate ulcerative lesions or exacerbate mucositis.
3. Chemical Burns from Fluoride or Acidic Rinses
Concentrated fluoride varnish applied without proper isolation may cause superficial burns, especially in children. Similarly, acidic mouthwashes (e.g., those containing high ethanol content) can erode the mucosal barrier, leading to hyperkeratotic patches.
4. Allergic or Sensitivity Reactions
Some individuals react to additives like propylene glycol, flavoring agents, or chlorhexidine itself, resulting in contact stomatitis-a red, itchy lesion that can mimic early aphthous ulcers.
These pathways highlight why a one‑size‑fits‑all prophylaxis protocol can backfire. The key is assessing patient‑specific risk factors before selecting a preventive regimen.
Who Is Most at Risk?
Certain patient profiles carry a higher likelihood of developing lesions after standard prophylactic care:
- Immunocompromised individuals - HIV, chemotherapy, organ transplant recipients.
- Patients with xerostomia - caused by medications (anticholinergics, antidepressants) or Sjögren’s syndrome.
- Elderly patients - thinner mucosa, polypharmacy, reduced manual dexterity.
- Children - especially those who cannot spit out rinses properly.
- Patients on bisphosphonate therapy - increased susceptibility to osteonecrosis and mucosal breakdown after scaling.
For these groups, clinicians should consider gentler mechanical techniques, lower‑concentration mouthwashes, or alternative agents such as essential oil blends that carry a reduced risk of fungal overgrowth.
Practical Recommendations to Minimize Lesion Risk
- Individualize the prophylaxis plan. Conduct a thorough medical history, focusing on immune status, medication list, and salivary flow.
- Choose the right chemical adjunct. For patients prone to candidiasis, prefer alcohol‑free essential oil rinses over chlorhexidine, or limit chlorhexidine to short‑term 2‑week courses.
- Limit mechanical trauma. Use low‑speed hand instruments for delicate tissues, and employ water cooling to reduce heat.
- Monitor fluoride application. Apply varnish only on enamel surfaces and protect soft tissues with a barrier (e.g., petroleum jelly) during treatment.
- Educate patients on signs of lesions. Provide a simple checklist: persistent soreness > 7 days, white patches that don’t scrape off, or any new ulcer.
- Schedule follow‑up examinations. Re‑evaluate lesion status at the next 3‑month prophylaxis visit, especially after changes in systemic health.
These steps help maintain the protective benefits of prophylaxis while keeping lesion rates low.
Comparison of Common Prophylactic Methods
| Method | Primary Goal | Typical Lesion Risk | Best‑Fit Patient Group |
|---|---|---|---|
| Mechanical scaling (ultrasonic) | Remove supra‑ and sub‑gingival plaque | Low‑to‑moderate (thermal irritation, micro‑ulcers) | Patients with healthy mucosa, good healing response |
| Chemical rinse - chlorhexidine 0.12% | Antimicrobial control for periodontal therapy | Moderate (candidiasis, taste alteration, mucosal staining) | Short‑term use in acute periodontal flare, not for xerostomia |
| Alcohol‑free essential‑oil rinse | Broad‑spectrum antibacterial with minimal irritation | Low (rare allergic contact) | Patients prone to fungal overgrowth or dry mouth |
| Fluoride varnish (5% NaF) | Enamel remineralization, caries prevention | Low (possible minor chemical burn if misapplied) | Children, high‑caries adults, patients with enamel hypoplasia |
The table illustrates that no single method is universally safe. Matching the right tool to the right patient dramatically cuts lesion incidence.
Frequently Asked Questions
Can regular dental cleanings cause mouth ulcers?
Yes, especially if the practitioner uses high‑speed instruments on delicate tissue or if the patient has a condition that slows healing, such as diabetes or bisphosphonate therapy. Using low‑speed tools and gentle pressure reduces this risk.
Is chlorhexidine safe for long‑term use?
Chlorhexidine is effective for short‑term plaque control, but prolonged use (beyond 2‑4 weeks) can disrupt the oral microbiome, leading to candidiasis and taste disturbances. For chronic needs, an alcohol‑free essential‑oil rinse is a better option.
Why do some patients develop white patches after fluoride treatment?
High‑concentration fluoride can cause a mild chemical burn on the mucosa, appearing as a white, slightly raised area. Proper isolation of soft tissue during application eliminates this side effect.
What signs should I look for to spot a developing oral lesion early?
Watch for persistent redness, ulceration lasting more than a week, white patches that don’t scrape off, or any new lump that feels firm. If any of these appear, schedule a dental or medical evaluation promptly.
Are there natural alternatives to chemical mouthwashes that won’t cause lesions?
Yes. Diluted (1:1) hydrogen peroxide, salt‑water rinses, and essential‑oil blends (e.g., thymol, eucalyptol) have antimicrobial properties with a lower risk of fungal overgrowth. They’re especially useful for patients with dry mouth.
Next Steps for Clinicians and Patients
For dental professionals, the take‑away is simple: perform a risk assessment before prescribing any prophylactic regimen. Document salivary flow, medication history, and any previous lesion episodes. For patients, stay alert to changes in the mouth and report them early; even a tiny sore can be a signal that the preventive plan needs tweaking.
By aligning preventive care with individual risk profiles, we keep the benefits of prophylaxis-clean teeth, healthy gums, and fewer cavities-while steering clear of the unintended side‑effect: oral lesions.


Debra Cine
October 3, 2025 AT 16:11Great overview, thanks for sharing! 😊
Rajinder Singh
October 9, 2025 AT 08:06The exposition on prophylactic modalities is commendable, yet one must consider the inherent paradox wherein interventions intended for preservation may, under specific systemic conditions, precipitate mucosal compromise. A measured analysis of patient history remains indispensable.
Samantha Leong
October 15, 2025 AT 05:46I appreciate the thoroughness of the risk assessment tool. It clearly outlines how each prophylactic choice can impact vulnerable patients. The sections on microbiome disruption and chemical burns are especially useful for clinicians. Keeping an eye on those side‑effects will help us intervene early.
Taylor Van Wie
October 21, 2025 AT 00:40Stop sugar‑coating the dangers-if you keep blasting patients with high‑speed scalers, you’re just digging a bigger hole for lesions. Americans need to hear the truth, not your polite dentistry PR.
carlee Lee
October 26, 2025 AT 18:33Tailoring the prophylaxis plan saves time and reduces risk.
Let’s keep it simple for patients.
chuck thomas
November 1, 2025 AT 13:26Exactly, a personalized approach is the most efficient route. When we align the chosen method with the patient’s salivary flow and immune status, we not only safeguard oral tissues but also improve compliance. It’s a win‑win, and the data you presented supports that notion nicely.
Gareth Pugh
November 7, 2025 AT 08:20Imagine the symphony of flavors when a gentle essential‑oil rinse replaces a harsh chlorhexidine splash-pure poetry for the palate and the microbiome alike.
Illiana Durbin
November 13, 2025 AT 03:13The recommendation to use barrier agents during fluoride varnish is practical and often overlooked. Applying petroleum jelly can prevent those pesky chemical burns. Simple steps like this make a big difference in patient comfort.
Tyler Heafner
November 18, 2025 AT 22:06The guidelines presented are exemplary of best practices in contemporary dentistry. By adhering to individualized prophylactic regimens, clinicians can mitigate iatrogenic lesions while preserving oral health. Rigorous documentation of patient risk factors is essential.
anshu vijaywergiya
November 24, 2025 AT 17:00Bravo for shedding light on the hidden perils of over‑aggressive prophylaxis! 🌟 Your emphasis on patient education transforms a sterile protocol into an empowering journey. When patients recognize early lesion signs, they become active participants in their own care.
ADam Hargrave
November 30, 2025 AT 11:53Ah, the eternal love‑hate affair with chlorhexidine-your article captures the drama perfectly 😂. Short‑term use is fine, but long‑term? That’s when the oral flora starts staging a revolt. Keep the rinse brief, and the microbes will stay on your side.
Michael Daun
December 6, 2025 AT 06:46nice breakdown of risk levels but dont forget to ask about med history before scaling
Rohit Poroli
December 12, 2025 AT 01:40From a clinical informatics perspective, integrating this risk calculator into electronic health records can streamline decision‑making. Leveraging data analytics to flag high‑risk profiles before the appointment will reduce lesion incidence. It’s a synergistic approach that merges preventive dentistry with health‑IT.
William Goodwin
December 17, 2025 AT 20:33💥 What a spectacular fusion of science and patient‑centered care! The vivid analogies you used make the recommendations memorable. If more clinicians embraced this holistic mindset, we’d see a dramatic decline in lesion‑related complications.
Isha Bansal
December 23, 2025 AT 15:26While the article admirably delineates the spectrum of prophylactic interventions, it is incumbent upon the practitioner to scrutinize each recommendation through the prism of individual patient pathology, thereby averting the inadvertent propagation of iatrogenic lesions. For instance, the indiscriminate application of high‑concentration fluoride varnish without proper soft‑tissue isolation may precipitate superficial chemical burns, a nuance that warrants explicit emphasis in clinical protocols. Moreover, the microbial dysbiosis engendered by prolonged chlorhexidine usage cannot be overstated; the resultant opportunistic overgrowth of Candida species often masquerades as benign aphthous ulcerations, yet may evolve into more recalcitrant forms of oral candidiasis if left unchecked. In patients with xerostomia, the diminished salivary buffering capacity synergistically amplifies the erosive potential of acidic adjuncts, necessitating the judicious selection of alcohol‑free rinses. Equally pertinent is the consideration of bisphosphonate therapy, where even low‑velocity mechanical debridement may culminate in osteonecrotic sequelae, underscoring the imperative for minimally invasive instrumentation techniques. The integration of a comprehensive risk‑assessment matrix, as outlined, constitutes a laudable stride toward personalized dental prophylaxis, though its efficacy is contingent upon meticulous data acquisition, including medication review, systemic disease burden, and prior lesion history. It is advisable for clinicians to document these variables within an interoperable digital framework, thereby facilitating longitudinal monitoring and iterative risk recalibration. Lastly, patient education remains a cornerstone of preventive dentistry; furnishing individuals with a concise yet thorough checklist of lesion warning signs empowers them to seek timely professional intervention, ultimately curbing disease progression. By harmonizing evidence‑based prophylactic modalities with individualized risk stratification, the dental community can uphold the dual mandate of disease prevention and iatrogenic harm mitigation.