
When you walk into a doctor’s office with a prescription in hand, do you feel like you’re being told what to take-or asked what you want? For too many people, the answer is still the former. But a quiet revolution is happening in healthcare: medication autonomy is shifting power from the provider to the patient. It’s not just about saying yes or no to a pill. It’s about understanding your options, weighing how a drug affects your life, and having the space to choose what fits you-not just what works on paper.
Why Medication Autonomy Isn’t Just a Nice Idea
Autonomy in medication selection isn’t new, but it’s finally being taken seriously. The idea traces back to the Nuremberg Trials after World War II, where forced medical experiments led to the first global rules about consent. By 1972, U.S. courts ruled that doctors must give patients all the material risks before treatment. Today, that means you have the right to know not just what a drug does, but how it might change your sleep, sex life, wallet, or daily routine. The real shift? Medicine is moving from “take this” to “what matters to you?” A 2023 report from the Agency for Healthcare Research and Quality found that 87% of U.S. hospitals now have formal shared decision-making protocols. But here’s the catch: only 42% of rural clinics actually use them. That gap isn’t just logistical-it’s ethical. If you’re told a drug will help your blood pressure but you’re worried about the dizziness that comes with it, and no one asks, you’re not being heard.What Makes Medication Choice Different from Other Medical Decisions
Choosing surgery is a one-time event. You say yes, you get cut, you recover. Medication? It’s ongoing. You take it every day, sometimes for years. And every time you swallow a pill, you’re making a choice-consciously or not. That’s why medication autonomy is more complex. Unlike a diagnostic scan, where the risk is temporary, drugs live inside you. A 2022 JAMA survey showed 73% of patients worry more about side effects from pills than from tests. Sexual dysfunction from SSRIs? Affects 25-30% of users. Monthly cost of a brand-name biologic? $5,000 to $7,000. And if you can’t afford it, you skip doses. That’s not noncompliance-it’s survival. And then there’s the influence of advertising. The FDA reports that 28% of patients ask for specific drugs after seeing direct-to-consumer ads. That’s not necessarily bad-if it starts a conversation. But if the doctor dismisses it, trust breaks down. Patients start feeling like their input doesn’t matter.How Doctors Are Learning to Listen
Changing how doctors talk about meds isn’t easy. It takes time, training, and a willingness to sit through silence. A 2023 study in Medical Education found it takes clinicians 12 to 18 months of deliberate practice to get good at shared decision-making. That means learning how to ask: “What are your biggest concerns?” or “What would make this treatment worth it for you?” Tools like the MacArthur Competence Assessment Tool (MacCAT-T) help doctors check if a patient truly understands their options-not just whether they can say “yes.” The Aid to Capacity Evaluation (ACE) is another simple tool used in clinics to spot when someone might need more support to make a decision. And it’s working. Patients who help choose their meds are 82% more likely to stick with them, compared to 65% when the doctor picks for them. That’s not just about compliance-it’s about dignity. One palliative care physician shared on Reddit how a cancer patient refused opioids because of her religious beliefs. Instead of pushing, they built a pain plan around her values-even if it meant more frequent dosing.The Hidden Barriers: Cost, Culture, and Time
Autonomy sounds great-until you hit reality. Three big barriers stand in the way: First, money. In 2023, 32% of Medicare Part D users changed or skipped meds because of cost. If your doctor prescribes a $6,000-a-month drug and you’re on a fixed income, autonomy doesn’t mean much if you can’t afford the choice. Second, culture. A 2023 survey found 35% of immigrant patients feel uncomfortable questioning their doctor’s advice. In some communities, doctors are seen as authorities-not partners. That’s not resistance; it’s respect. But it means autonomy tools must be culturally adapted, not just translated. Third, time. The average primary care visit is 15 minutes. Try explaining three medication options, their side effects, costs, and how they fit into someone’s life in that window. Impossible. That’s why pre-visit tools-like short online questionnaires that help patients think through their priorities-are gaining traction. One VA pilot cut decisional conflict by 42% just by giving patients time to reflect before the appointment.Who’s Doing It Right-and Who’s Falling Behind
Specialty matters. Psychiatrists and endocrinologists lead the pack, with 78% and 71% respectively using shared decision-making regularly. Why? Because their patients are often on long-term meds with heavy side effects. They’ve learned that forcing a drug doesn’t work. Emergency medicine? Only 43% of ER doctors use these practices. In a crisis, speed wins. But even there, autonomy can be part of the conversation: “We can give you this antibiotic now, but if you’re worried about stomach issues, we can wait 24 hours and see if it clears up.” Hospitals with patient advisory councils implement autonomy protocols 2.3 times faster. Academic medical centers hit 82% compliance. Community hospitals? Just 57%. The difference? Leadership that sees patients as partners, not problems.What’s Next: Digital Tools and Personalized Medicine
The future of medication autonomy isn’t just better conversations-it’s better tech. New software platforms, valued at $1.2 billion in 2023, are now built specifically for medication choice. They offer side-by-side comparisons of drugs, cost calculators, and even videos from other patients explaining their decisions. And then there’s pharmacogenomics. Testing your genes to see how you’ll react to a drug used to cost $1,200. Now it’s under $250. That means your next antidepressant might be chosen based on your biology-not guesswork. But here’s the risk: digital tools can deepen inequality. Nearly 4 in 10 adults over 65 say they struggle to use medication apps. If autonomy relies on smartphones and apps, we risk leaving behind the very people who need it most.
What You Can Do-Right Now
You don’t need to wait for the system to change. Here’s how to claim your right to choose:- Ask: “What are my options besides this one?”
- Ask: “What’s the most common side effect, and how does it affect daily life?”
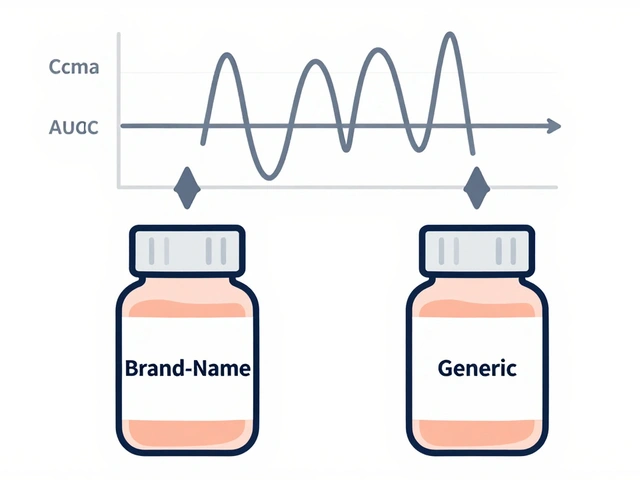
- Ask: “Is there a generic or cheaper version that works just as well?”
- Ask: “What happens if I don’t take this?”
- Bring a list of your values: “I need to be alert for work,” or “I can’t take something that messes with my sleep.”
When Autonomy Gets Messy
Some argue that too much autonomy can lead to bad choices. Dr. Arthur Caplan of NYU points out that 40% more people refused antibiotics in 2022-2023 after hearing misinformation online. That’s real. But the answer isn’t to take away choice-it’s to give better information. The Hastings Center calls this “medication exceptionalism”-where patients treat drugs differently than other treatments. Maybe it’s because of Big Pharma’s history of hiding side effects. Maybe it’s because pills feel like a loss of control. Either way, the solution isn’t paternalism. It’s transparency. The American Medical Association says doctors must not withhold appropriate meds based on assumptions about a patient’s income, race, or “adherence.” That’s crucial. If you’re poor, you still deserve access to the best options-not just the cheapest ones.Final Thought: Autonomy Is a Practice, Not a Moment
Medication autonomy isn’t a one-time signature on a form. It’s a series of conversations over months or years. It’s asking for alternatives when the first drug makes you nauseous. It’s pushing back when the cost is too high. It’s saying, “I’d rather try therapy first.” It’s messy. It’s hard. But it’s necessary. Because no algorithm, no guideline, no doctor can know what matters to you better than you do.Can I refuse a medication even if my doctor recommends it?
Yes. If you have decision-making capacity, you have the legal and ethical right to refuse any medication-even if your doctor believes it’s the best option. This right is protected under informed consent laws established in the U.S. since the 1972 Canterbury v. Spence case. Doctors must explain the risks of refusing, but they cannot force treatment.
What if I can’t afford my prescribed medication?
Cost should never be a barrier to choice. Ask your doctor for generic alternatives, patient assistance programs, or lower-cost biosimilars. Many pharmaceutical companies offer discount cards. Pharmacies can also help you compare prices across locations. If you’re on Medicare, check if your plan has a formulary exception process. You have the right to request a more affordable option that still treats your condition.
How do I know if I have the capacity to make a medication decision?
You have decisional capacity if you can understand the information about your medication, appreciate how it affects you, weigh the pros and cons, and communicate your choice clearly. Tools like the Aid to Capacity Evaluation (ACE) help doctors assess this. If you’re unsure, ask for a second opinion or a mental health evaluation. Capacity can change over time-especially with conditions like depression or dementia-but it’s not assumed based on age or diagnosis.
Are there medications I can’t refuse?
In most cases, no. Even for serious conditions like diabetes or hypertension, you can refuse treatment. Exceptions exist only in rare, legally defined emergencies-like when someone is a danger to themselves or others due to severe mental illness, and a court has authorized involuntary treatment. Outside of those extreme cases, your consent is required.
What if my doctor won’t discuss other options?
It’s a red flag. A doctor who refuses to discuss alternatives isn’t practicing patient-centered care. You can ask for a referral to another provider, seek a second opinion, or contact your insurance for a list of doctors who use shared decision-making tools. Many clinics now advertise this as a service. You deserve a partner in your care-not a director.

Meghan O'Shaughnessy
December 18, 2025 AT 01:20Finally someone gets it. I took my first antidepressant and it turned me into a zombie who couldn’t orgasm or remember her own birthday. My doctor said 'it's just side effects' like that's normal. It wasn't. I switched meds after six months of crying in the shower. Now I'm on a cheaper generic that lets me laugh again. Autonomy isn't luxury-it's survival.
Nishant Desae
December 18, 2025 AT 12:51in india we dont even get to choose what medicine to take, doctor just gives u a scrip and u pay and take it. sometimes the medicine is not even available in local pharmacy and u have to travel 50km. i had a friend who got prescribed a $3000/month drug for diabetes and his family sold their TV to buy it for 2 months. then he just stopped taking it. nobody asked why. they just said he was non compliant. but he was just poor. autonomy means nothing if you dont have money or access. also doctors here think patients are stupid. they dont explain anything. just say 'take this' and walk away. its sad.
Kaylee Esdale
December 18, 2025 AT 21:58My grandma refused her blood pressure med because it made her dizzy and she fell twice. Doctor called her noncompliant. I told him she’s 82, lives alone, and doesn’t want to die from a fall. We switched to a different med. She’s still alive. And she still makes her own damn choices. That’s not defiance. That’s wisdom.
CAROL MUTISO
December 19, 2025 AT 12:34Oh wow. So now we’re supposed to believe that doctors are just waiting to be asked nicely to stop treating us like cattle? Let me guess-the next step is having patients vote on whether antibiotics should be prescribed based on TikTok trends. 🙄 The fact that 28% of people ask for drugs because of ads is terrifying. And now you’re glorifying it as 'autonomy'? This isn’t empowerment. It’s pharmaceutical marketing dressed up as patient rights. I’ve seen people refuse insulin because they saw a YouTube video that said sugar is 'natural.' Autonomy without education is just dangerous.
Virginia Seitz
December 20, 2025 AT 19:11Yes. 👏 I asked for a cheaper pill. Got it. No drama. My body. My rules. 💊
Michael Whitaker
December 22, 2025 AT 18:11While I appreciate the sentiment, the notion of patient autonomy in pharmacotherapy is, in many respects, a bourgeois fantasy. In a system where the average primary care visit lasts 13.7 minutes (per NEJM 2022), and where 78% of physicians report burnout, the expectation that clinicians will engage in nuanced, value-based decision-making is not only unrealistic-it is ethically irresponsible to demand it without systemic reform. Autonomy without adequate infrastructure is performative.
Brooks Beveridge
December 23, 2025 AT 16:10Man, I used to think my doctor knew best. Then I got prescribed this weight-loss pill that made me feel like I was drunk all day. I said no. He didn’t argue. He just said 'what are you trying to get out of life?' and we talked for 20 minutes. Turned out I just wanted to sleep better. We switched to therapy and walking. Best decision I ever made. You don’t need to be loud to be heard. Just be honest.
Sachin Bhorde
December 24, 2025 AT 04:42bro the real issue is not autonomy its pharmacokinetics. most docs dont even know CYP450 metabolism pathways. i had a guy on fluoxetine and then got prescribed clarithromycin-CYP3A4 inhibition = serotonin syndrome risk. nobody checked. so yeah autonomy is cool but if your doc is a glorified script-writer with no clinical depth, you’re just gambling. get a pharmacist involved. they know more than your GP about drug interactions. also generics are not 'inferior'-they’re bioequivalent. stop buying brand names like they’re designer jeans.
Joe Bartlett
December 25, 2025 AT 14:49Autonomy? We used to just trust the doctor. Now everyone’s a YouTube MD. We don’t need more choices-we need more discipline. Take the pill. Stop complaining. This is why Britain’s NHS works better than your chaotic mess.
Marie Mee
December 27, 2025 AT 00:51they’re all lying. the drugs are designed to make you dependent. the side effects are intentional. they want you to need more pills. the FDA is owned by big pharma. i stopped all my meds. now i eat turmeric and breathe deep. my blood pressure is better. they’re scared of people waking up.
Kent Peterson
December 27, 2025 AT 20:1687% of hospitals have 'protocols'? That’s meaningless. Protocols are paperwork. Actual shared decision-making? Less than 10%. And let’s not pretend patients are rational actors-most can’t even read at a 6th-grade level. You can’t 'empower' someone who doesn’t know what 'bioequivalent' means. This whole article is a glossy PR piece for lazy doctors who don’t want to make decisions. The truth? Most patients want to be told what to do. They’re tired of responsibility.
Josh Potter
December 29, 2025 AT 19:45OMG YES. I asked my doc for a non-drowsy antihistamine and he laughed. Like I was asking for a unicorn. I went to another clinic. Got it. No more 3pm naps. My boss noticed. I got promoted. Autonomy isn’t radical. It’s just common sense. Also-why is everyone so scared to say 'I don’t know'? Just say it. We’ll wait.
Evelyn Vélez Mejía
December 30, 2025 AT 08:38The moral architecture of modern medicine is predicated upon the Kantian imperative of respect for persons. To deny patient autonomy is to reduce the individual to a mere instrument of clinical utility-a violation of the foundational covenant of medical ethics. The statistical outcomes cited (82% adherence) are merely epiphenomenal; the true value lies in the ontological recognition of the patient as an end-in-themselves. To reduce this to cost-efficiency metrics or behavioral compliance is to betray the very essence of healing.
Martin Spedding
December 30, 2025 AT 17:32Just say no to meds. That’s the real revolution. I didn’t take my statin. My cholesterol went up. My anxiety went down. My life improved. Who’s the real patient here? The one who obeys? Or the one who dares to say 'fuck this'? 🤷♂️