Waking up with a tingling sensation in your thumb or dropping your phone because your grip just failed you is more than just an annoyance. It’s often the first sign that something is wrong inside your wrist. This condition, known as Carpal Tunnel Syndrome, is a common disorder caused by pressure on the median nerve as it travels through the wrist. While many people assume this is simply "tech neck" or computer strain, the reality is far more mechanical. It involves a narrow passageway in your wrist getting crowded, leading to pain, numbness, and potentially permanent damage if ignored.
Understanding how this happens-and why nerve decompression is the surgical procedure used to relieve pressure on the median nerve-is crucial for anyone experiencing these symptoms. You don’t have to live with the discomfort. Whether you are dealing with mild tingling or severe weakness, there are clear paths to recovery. Let’s break down what is happening in your wrist, how doctors confirm the diagnosis, and when surgery becomes the best option.
What Is Happening Inside Your Wrist?
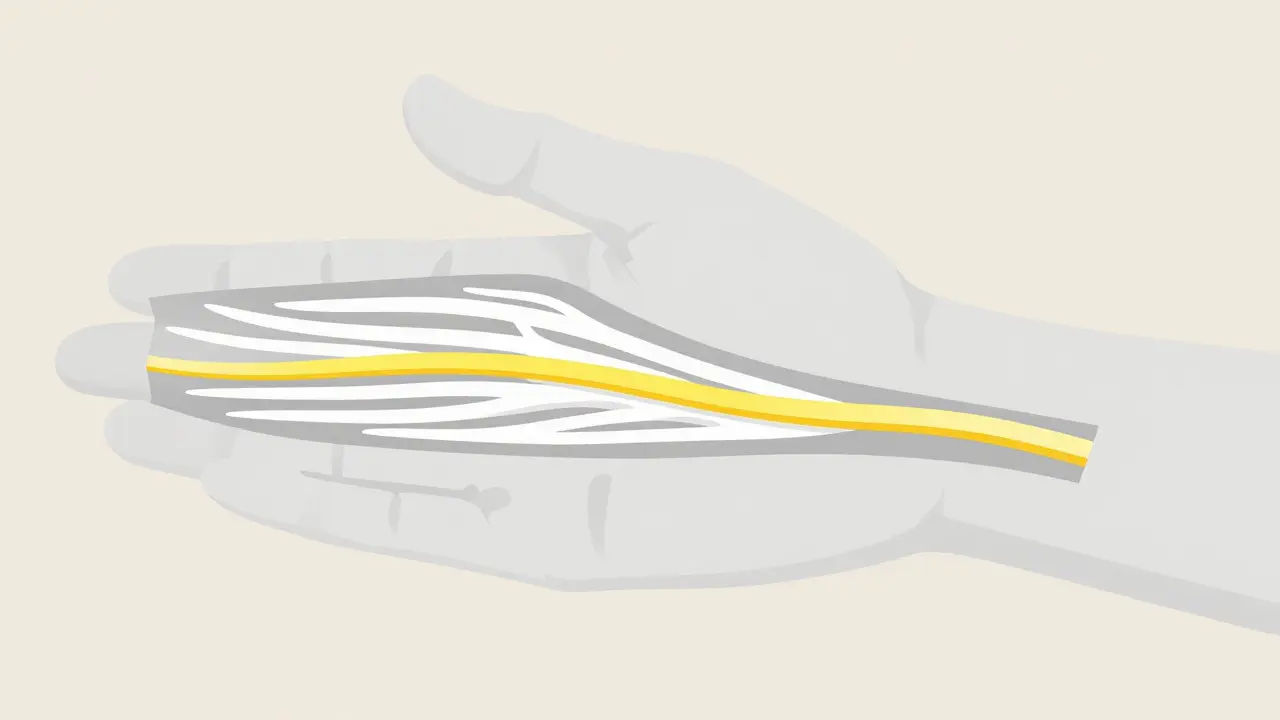
To understand why your hand hurts, you need to look at the anatomy. The carpal tunnel is a narrow channel in your wrist, about 1-2 cm wide. It acts like a tunnel bounded by bones on one side and a tough band of tissue called the transverse carpal ligament on the other. Inside this tight space, two things travel together: nine flexor tendons (which help you bend your fingers) and the median nerve is the major nerve supplying sensation to the thumb, index, middle, and half of the ring finger.
Normally, the pressure inside this tunnel is low, around 2-10 mmHg. But when inflammation occurs, or when the tendons swell due to repetitive motion or injury, that pressure spikes. When it exceeds 30 mmHg, the median nerve gets squeezed. Think of it like stepping on a garden hose; the water (nerve signals) can’t flow freely. This compression disrupts the blood supply within the nerve itself, leading to those familiar symptoms of numbness, tingling, and pain.
This isn’t just a modern office problem. While we often blame keyboards, research from the National Institute for Occupational Safety and Health (NIOSH) shows that forceful gripping motions-like using heavy tools or even vigorous typing with poor posture-are the real culprits. Interestingly, a 2023 review in the New England Journal of Medicine found no direct causal link between simple computer use and developing CTS, but high-force activities increase risk significantly.
Recognizing the Symptoms Early
Catching Carpal Tunnel Syndrome early makes treatment much easier. The symptoms usually start slowly and worsen over time. Here is what to look for:
- Numbness and Tingling: This typically affects the thumb, index finger, middle finger, and the radial half of the ring finger. Many patients describe it as pins and needles.
- Nighttime Pain: About 89% of patients report waking up at night with their hand asleep. Shaking the hand often provides temporary relief.
- Weakness: As the condition progresses, you might drop objects frequently. This is due to weakness in the muscles at the base of the thumb (thenar eminence).
- Pain Radiating Up the Arm: In some cases, the pain can shoot up the forearm toward the shoulder.
If you notice your thumb muscle shrinking or flattening, that is a sign of advanced nerve damage. At this stage, conservative treatments are less likely to work, and surgical intervention is almost always necessary to prevent permanent loss of function.
How Doctors Diagnose CTS
You cannot diagnose yourself accurately based on symptoms alone. Other conditions, like arthritis or cervical radiculopathy (pinched nerve in the neck), can mimic CTS. A proper diagnosis requires objective testing.
The gold standard for diagnosis is nerve conduction studies are electrodiagnostic tests that measure how fast electrical impulses move through your nerves. These tests check if the median nerve is slowed down or blocked. According to standards set by the American Association of Neuromuscular & Electrodiagnostic Medicine, abnormal results include distal motor latency exceeding 4.2 milliseconds or sensory conduction velocity below 45 m/s.
Doctors may also perform physical exams, such as Tinel’s sign (tapping over the nerve to see if it causes tingling) or Phalen’s maneuver (bending the wrist to reproduce symptoms). However, electrodiagnostic testing is critical before considering surgery, as it confirms the severity of the compression in 85-95% of surgical candidates.

Non-Surgical Treatments: What Works First?
For mild to moderate cases, especially those lasting less than three months, non-surgical options are highly effective. Studies show a 70% success rate for conservative management in early-stage CTS.
- Nocturnal Splinting: Wearing a wrist brace at night keeps your wrist in a neutral position, preventing the bending that increases pressure in the tunnel. Research indicates this reduces symptoms by 40-60% in short-term cases. The key is consistency; wearing it for 6-8 hours nightly is essential.
- Corticosteroid Injections: Injecting anti-inflammatory steroids directly into the carpal tunnel can provide significant relief for 3-6 months. About 60-70% of patients find this helpful. However, repeated injections may lead to tissue fibrosis, which could complicate future surgery, so they are usually limited to one or two attempts.
- Activity Modification: Changing how you work is vital. If you do repetitive gripping, take frequent breaks. Ergonomic assessments can help adjust your workstation to keep your wrists straight, reducing extension beyond 15 degrees.
If these methods fail after 6-8 weeks, or if your symptoms are already severe (constant numbness or muscle wasting), waiting longer rarely helps. Delaying treatment allows nerve damage to become permanent.
Nerve Decompression Surgery: The Definitive Solution
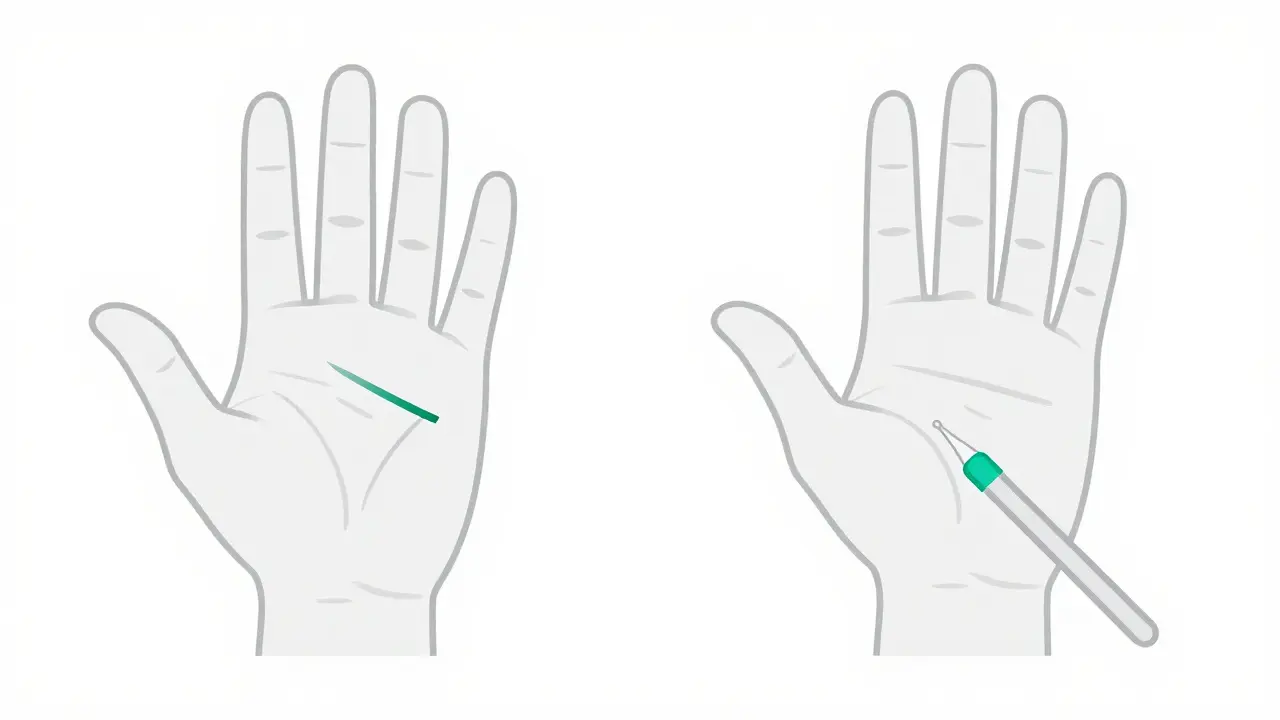
When conservative measures fail, carpal tunnel release surgery is a procedure that cuts the transverse carpal ligament to create more room for the median nerve. This is not a minor fix; it is a structural change that permanently relieves pressure.
There are two main approaches:
| Feature | Open Carpal Tunnel Release | Endoscopic Carpal Tunnel Release |
|---|---|---|
| Incision Size | Larger incision in the palm | One or two small incisions |
| Recovery Time | Slower; return to desk work in 2-4 weeks | Faster; return to desk work in 1-2 weeks |
| Long-Term Outcomes | Highly effective (75-90% success) | Equally effective at 6+ months |
| Risk Profile | Lower risk of incomplete release | Slightly higher risk of nerve injury if surgeon lacks experience |
| Cost | Generally lower | Higher due to specialized equipment |
Open surgery remains the most common method, accounting for 90% of procedures. It has a proven track record and lower complication rates regarding nerve injury. Endoscopic surgery offers a quicker initial recovery but requires a surgeon with specific training. Both methods achieve similar long-term relief, with 75-90% of patients reporting significant improvement.
Recovery and Realistic Expectations
Surgery is not a magic switch. While the pressure on the nerve is relieved immediately, the nerve itself needs time to heal. Most patients feel immediate relief from nighttime pain, but full recovery takes patience.
Here is what the timeline typically looks like:
- Weeks 1-2: Keep the wound dry. Perform gentle finger exercises to prevent stiffness. Sutures are removed around day 10-14.
- Weeks 3-4: Scar massage begins. Light activities resume. You may still experience some numbness or tingling as the nerve regenerates.
- Weeks 6-8: Grip strength returns gradually. Most desk workers are fully back to normal. Manual laborers may need up to 12 weeks.
A common complaint post-surgery is "pillar pain," a deep ache in the thenar and hypothenar muscles. This affects 15-30% of patients but usually resolves within a few months. Smoking slows this process significantly; smokers experience 30% slower recovery times. Managing diabetes is also critical, as high blood sugar impedes nerve healing.
Preventing Recurrence
Surgery fixes the current problem, but it doesn’t make you immune to future issues. If your job involves repetitive forceful gripping, your risk of recurrence is higher. Assembly line workers, for example, have a 45% recurrence rate compared to 15% in those with non-repetitive jobs.
To protect your wrists long-term:
- Maintain a healthy weight. Obesity increases CTS risk by 2.3-fold.
- Use ergonomic tools. Anti-vibration gloves and padded handles reduce stress on the tendons.
- Take micro-breaks. Every 20 minutes, stretch your hands and wrists.
- Monitor blood sugar if you have diabetes. Keeping HbA1c below 7% supports better nerve health.
Does Carpal Tunnel Syndrome go away on its own?
In rare cases, such as during pregnancy, CTS may resolve spontaneously within three months postpartum due to fluid retention decreasing. However, for the general population, CTS is progressive. Without treatment, the compression worsens, leading to permanent nerve damage. Early intervention is key to preventing chronic issues.
Is carpal tunnel surgery painful?
The surgery itself is performed under anesthesia, so you feel no pain during the procedure. Post-operatively, most patients report manageable soreness and swelling. Pillar pain, a deep ache in the palm muscles, is common but temporary. Over-the-counter pain relievers are usually sufficient for the first week.
How long does it take to recover from carpal tunnel release?
Recovery varies by occupation. Desk workers typically return to work within 1-2 weeks for endoscopic surgery and 2-4 weeks for open surgery. Full grip strength and complete resolution of numbness can take 6-12 weeks. Manual laborers may require up to 12 weeks for full recovery.
Can I type immediately after carpal tunnel surgery?
You should avoid typing for at least the first week to allow the incision to heal and reduce swelling. After suture removal (around 10-14 days), you can gradually reintroduce typing, starting with short sessions. Use an ergonomic keyboard and take frequent breaks to prevent re-aggravation.
What are the risks of carpal tunnel surgery?
Complications are rare, occurring in 1-5% of cases. Potential risks include infection, scar tenderness (20%), pillar pain (15-30%), and very rarely, injury to the median nerve or its branches (0.5-2%). Choosing an experienced hand surgeon minimizes these risks significantly.