When you feel a sharp, shooting pain down your arm or leg, it’s not just a muscle cramp. It could be radiculopathy - a nerve root problem that’s more common than you think. Cervical radiculopathy affects the neck and arms, while lumbar radiculopathy hits the lower back and legs. Together, they account for 95% of all nerve root issues. The good news? Most people get better without surgery. But only if they know what’s really going on - and how to treat it right.
What Exactly Is Radiculopathy?
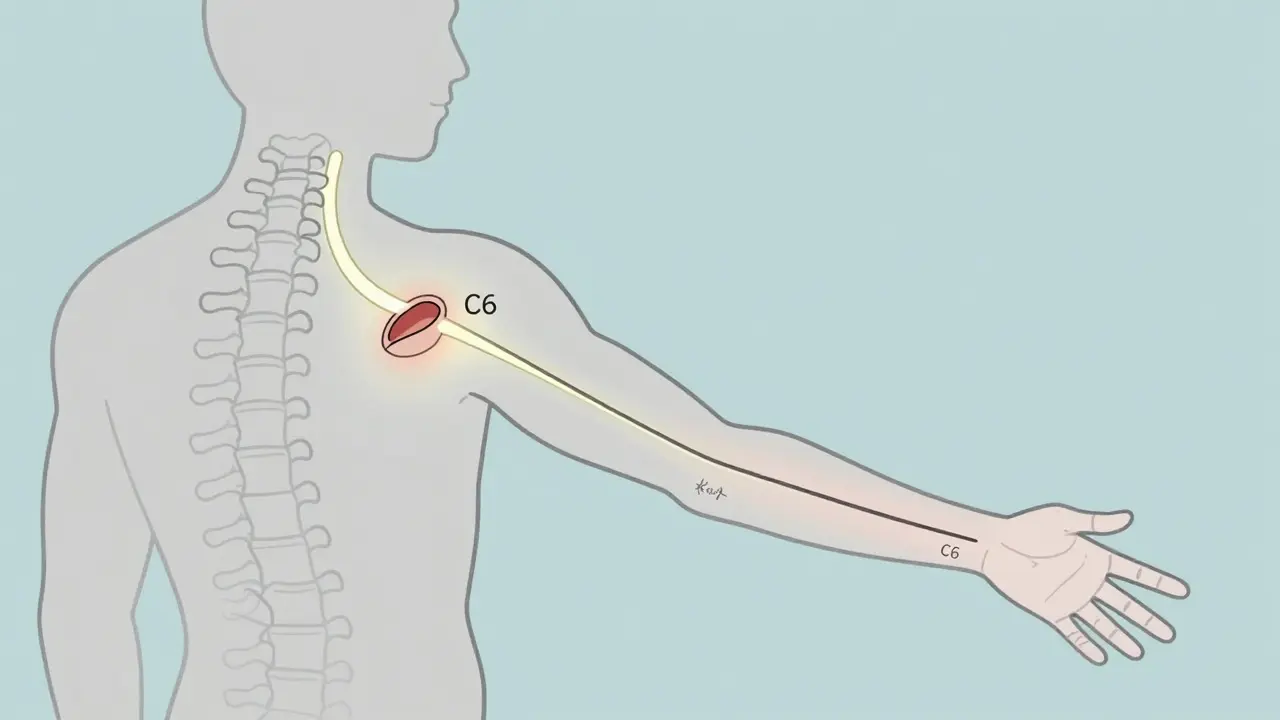
Radiculopathy happens when a nerve root gets pinched, irritated, or compressed as it leaves your spine. Think of it like a garden hose kinked near the spigot. The water (nerve signals) can’t flow properly, so the end (your arm, hand, leg, or foot) starts to hurt, tingle, or go weak. It’s not just back pain - it’s nerve pain that follows a specific path. In the neck (cervical spine), the most common culprits are C6 and C7. If C6 is compressed, you’ll feel pain along your thumb and index finger, and your biceps might feel weak. If C7 is affected, the middle finger goes numb, and you’ll struggle to straighten your elbow. In the lower back (lumbar spine), L5 and S1 are the usual suspects. L5 compression causes foot drop - your foot slaps the ground when you walk. S1 irritation sends pain from your butt down the back of your calf to the sole of your foot. The cause depends on age. Under 50? It’s usually a herniated disc. Over 50? It’s more likely bone spurs or narrowing of the nerve tunnel from arthritis. A 2023 study from the Cleveland Clinic found that 78% of cervical radiculopathy cases in older adults come from degenerative changes, not sudden injuries.Why Cervical and Lumbar Are Different
Even though both involve pinched nerves, they behave differently. Cervical radiculopathy tends to heal faster. About 89% of cases improve with conservative care within six months. Lumbar radiculopathy? Only 76% improve in that time. Why the gap? For one, the lumbar spine carries your whole body weight. Every step, every twist, every lift adds pressure to those nerves. People with lumbar radiculopathy also report higher disability scores. A 2022 study in the Journal of Orthopaedic Research found that on the Oswestry Disability Index (a standard pain and function scale), lumbar patients scored 37% higher than cervical patients. Their recovery took 28% longer - about 14 weeks versus 11. Work matters too. Lumbar radiculopathy is strongly tied to heavy lifting. One study showed workers who lift regularly are over three times more likely to develop it. Cervical cases, on the other hand, are more linked to trauma - car accidents, falls, or sudden jerks.What Does Treatment Look Like?
The first rule? Don’t rush to surgery. The American College of Physicians recommends trying 6 to 8 weeks of conservative care before even thinking about it. And most people don’t need surgery. About 85% of cases resolve on their own with time and the right rehab. Start with rest and anti-inflammatories. Ibuprofen (400mg three times a day) for a few days can reduce swelling around the nerve. But don’t just sit still. Movement is key. Studies show that people who stay active recover faster than those who bed rest. Physical therapy is the cornerstone. For cervical radiculopathy, gentle traction - using a light weight (5-10 lbs) to stretch the neck - helps open space around the nerve. Then, exercises like chin tucks and scapular retractions strengthen the muscles that support your spine. One patient survey found 78% satisfaction with these specific moves. For lumbar radiculopathy, McKenzie extension exercises are gold standard. Lie on your stomach, prop yourself up on your elbows, then slowly push your upper body up. This moves the disc away from the nerve. Core stability work - planks, bird-dogs, glute bridges - is equally important. You need strong abs and hips to take pressure off the lower back.The Hidden Problem: Inconsistent Rehab
Here’s where most people fail. They do PT for six weeks, feel better, and stop. Big mistake. Research shows that patients who stick to their home exercises recover 47% faster. Consistency beats intensity. Ten minutes a day, seven days a week, is better than an hour once a week. Another pitfall? Bad pillows. If you sleep with your neck twisted or too high, you’re re-injuring the nerve every night. A thin, supportive pillow that keeps your head aligned with your spine makes a huge difference. For lower back pain, sleeping on your side with a pillow between your knees helps reduce pressure. Workplace habits matter too. If you sit all day, adjust your chair so your knees are level with your hips. Use a lumbar roll. Take a five-minute walk every hour. One study found that ergonomic tweaks cut symptoms by 32% in office workers.When Injections Help - and When They Don’t
Epidural steroid injections are popular. Doctors offer them. Patients hope for miracles. But the evidence is mixed. The Cochrane Database says they give only short-term relief - maybe two to six weeks. After that? No better than placebo. Yet in real-world practice, 58% of pain specialists say they see real, lasting improvement. Why the gap? Maybe because injections work best for people with clear inflammation, not just mechanical compression. If your MRI shows swelling around the nerve, injections might help. If it’s just a bone spur pinching the nerve? Probably not. One thing’s clear: injections aren’t a cure. They’re a bridge. They buy you time to do the real work - rehab.What Doesn’t Work
Many patients try quick fixes - massage, chiropractic adjustments, traction machines bought online. Some help. Some don’t. But here’s what consistently fails:- Returning to heavy lifting too soon - causes 28% of symptom recurrences
- Skipping home exercises - 61% of non-responders admit they didn’t do them
- Waiting too long to start rehab - every week of delay makes recovery harder
- Believing pain = damage - pain can linger even after the nerve heals

New Tools, Better Outcomes
In January 2023, the FDA approved MedoScan RAD - an AI tool that analyzes MRIs and spots nerve compression with 96.7% accuracy. That’s up from 89% with human reading alone. This means faster, more precise diagnoses. The NIH is running a trial called RAD-REHAB, testing personalized rehab based on exactly which nerve is affected. Early results? Patients improved 41% more than those on standard programs. Instead of one-size-fits-all, you get a plan built for your specific nerve damage. Emerging treatments like targeted steroid nanoparticles show promise - 78% pain reduction in early trials. Platelet-rich plasma (PRP) is being tested too, but there’s still not enough proof it works. Stick with what’s proven: movement, strength, consistency.Real Recovery: What to Expect
You won’t feel better overnight. But you will feel better. Eighty-two percent of patients return to their normal activities within a year. Only 8% develop long-term pain. That’s hopeful. Recovery isn’t linear. Some days are good. Some days hurt more. That’s normal. What matters is that you keep moving. Keep doing your exercises. Keep adjusting your posture. Keep listening to your body. The data is clear: if you start early, stick with rehab, and avoid the traps, your odds of full recovery are excellent. You don’t need surgery. You don’t need magic. You just need a plan - and the discipline to follow it.Can cervical radiculopathy cause headaches?
Cervical radiculopathy doesn’t directly cause headaches. But if nerve irritation in the upper neck (C1-C3) triggers muscle tightness or referred pain, you might feel tension-type headaches. These usually feel like a band of pressure around the head, not the sharp, shooting pain of nerve compression. If headaches are your main symptom, other causes like migraines or TMJ should be ruled out.
Is lumbar radiculopathy the same as sciatica?
Yes - sciatica is the most common form of lumbar radiculopathy. It specifically refers to pain along the sciatic nerve, which runs from the lower back down the leg. Most cases are caused by compression of the L5 or S1 nerve roots. Not all leg pain is sciatica, though. Other conditions like hip arthritis or hamstring strains can mimic it. An MRI or nerve test can confirm the diagnosis.
How long should I wait before seeing a doctor?
If pain lasts more than two weeks, or if you notice weakness, numbness, or loss of bladder/bowel control, see a doctor immediately. Waiting too long can delay recovery. But if the pain is mild and improving, give it 6-8 weeks of rest, gentle movement, and over-the-counter pain relief before seeking advanced care. Most cases resolve on their own with time.
Can I still exercise with radiculopathy?
Yes - but not all exercises. Avoid heavy lifting, twisting, or high-impact activities like running or jumping. Focus on low-impact movement: walking, swimming, stationary biking. Gentle stretching and core exercises are encouraged. Pain should never increase during or after exercise. If it does, stop and recheck your form or consult a physical therapist.
Do I need an MRI to diagnose radiculopathy?
Not always. A skilled physical therapist or doctor can often diagnose radiculopathy through movement tests and symptom patterns. An MRI is recommended if symptoms don’t improve after 6 weeks, if there’s progressive weakness, or if surgery is being considered. MRI shows the exact location and severity of nerve compression - but it’s not needed for every case.




Dylan Patrick
March 14, 2026 AT 21:32Been there. Cervical radiculopathy hit me hard after a car wreck. Thought it was just a stiff neck. Turns out, my C6 was screaming. PT saved me - not surgery, not pills. Just consistent chin tucks and sleeping on a thin pillow. No magic. Just discipline.
Now I do 10 minutes a day, every day. Even on vacation. Even when it hurts. That’s the secret.
Kandace Bennett
March 15, 2026 AT 17:31OMG I KNEW IT 😤
Like, duh, of COURSE lumbar radiculopathy is worse - we’re talking about the spine that carries your whole body weight 😭
And people still think a $20 traction device from Amazon fixes everything?? 🤦♀️
Also, if you’re not doing McKenzie extensions, you’re just vibing with pain. Sorry, not sorry.
Tim Schulz
March 16, 2026 AT 01:14Oh wow, another ‘just move more’ post. Groundbreaking. 🙄
Let me guess - you also believe in eating kale and drinking lemon water to cure cancer?
Real talk: if your ‘rehab’ is just doing bird-dogs while your disc is herniated 8mm, you’re not healing - you’re just doing yoga for masochists.
Also, FDA-approved AI? Cool. But I’m still waiting for the FDA to approve that my sciatica isn’t caused by alien mind control.
Jinesh Jain
March 16, 2026 AT 06:52Interesting. In India, many people don’t even get diagnosed. They just live with it. Some use traditional massage. Others wait until they can’t walk. I wonder how many avoid PT because of cost or access. Maybe the real issue isn’t the rehab - it’s the system that makes it hard to get to rehab.
douglas martinez
March 16, 2026 AT 11:18While the article provides a comprehensive overview, I must emphasize the importance of clinical correlation. Radiographic findings do not always align with symptomatology. A patient may exhibit significant degenerative changes on MRI yet remain asymptomatic, while another with minimal findings may experience severe radiculopathy. A multidisciplinary approach involving physical therapy, pain psychology, and neurology is essential for optimal outcomes.
Sabrina Sanches
March 17, 2026 AT 12:40I just started my exercises!!!
And I’m crying because I did 3 bird-dogs and my back felt like it was on fire
But I did it!!!
And I’m proud
And I’m gonna do it again tomorrow
And the next day
And the next
And I’m not giving up
EVER
Shruti Chaturvedi
March 19, 2026 AT 10:33Now I do my planks every morning
And I sleep with a pillow between my knees
And I walk every hour
It’s not glamorous
But it works
Katherine Rodriguez
March 20, 2026 AT 04:56So let me get this straight - you’re telling me the government and big pharma are hiding the real truth?
Because I’ve been doing all this PT and posture stuff for months
And I still can’t sit without screaming
So maybe the real problem is not that I’m lazy
But that the whole system is rigged
And they don’t want us to heal
Just keep taking pills
Devin Ersoy
March 20, 2026 AT 13:44Let’s be real - this whole ‘conservative care’ thing is just a glorified waiting game.
You know what’s really going on? The spine is a biological Rube Goldberg machine held together by duct tape and hope.
And yeah, McKenzie exercises? Sure, they’re cute.
But have you ever tried a 20-minute inversion table session while listening to binaural beats and whispering affirmations to your L5 disc?
That’s real healing.
Also, I’m 100% sure the FDA’s AI tool is just a front for NSA data harvesting. Just saying.
Scott Smith
March 21, 2026 AT 07:06Consistency is everything. I’ve seen patients who do five minutes a day, seven days a week, outperform those who do an hour once a week. It’s not about intensity - it’s about repetition. The body remembers. The nervous system adapts. You don’t need fancy gear. You don’t need a trainer. You just need to show up. Every day.
Dylan Patrick
March 22, 2026 AT 06:05Replying to @douglas martinez - I hear you. But in real life, most people don’t have access to multidisciplinary teams. They have a 15-minute doc visit and a $500 copay. That’s why the simple stuff - posture, pillow, 10-minute home routine - matters more than ever. Real healing happens in the gaps.
Sabrina Sanches
March 22, 2026 AT 20:32Replying to @Shruti Chaturvedi - YES. I did the same thing. Walked every hour. Changed my chair. Slept with a pillow between my knees. Three months later, I ran a 5K. Not because I was brave. Because I was consistent. You’re not alone.