Steroid Injection Risk Calculator
Personal Information
Injection History
Surgery Plans
When you have painful knees or hips from osteoarthritis, a steroid injection can feel like a miracle. You walk in stiff and sore, and within a few days, you’re moving better, feeling less pain, maybe even back to your daily routine. It’s quick, it’s common - over 12 million of these injections are done every year in the U.S. alone. But here’s something most patients never hear: intra-articular steroid injections aren’t just local. They don’t stay in the joint. And what happens in your bloodstream after that shot might be more dangerous than you think.
What Happens After the Needle Goes In?
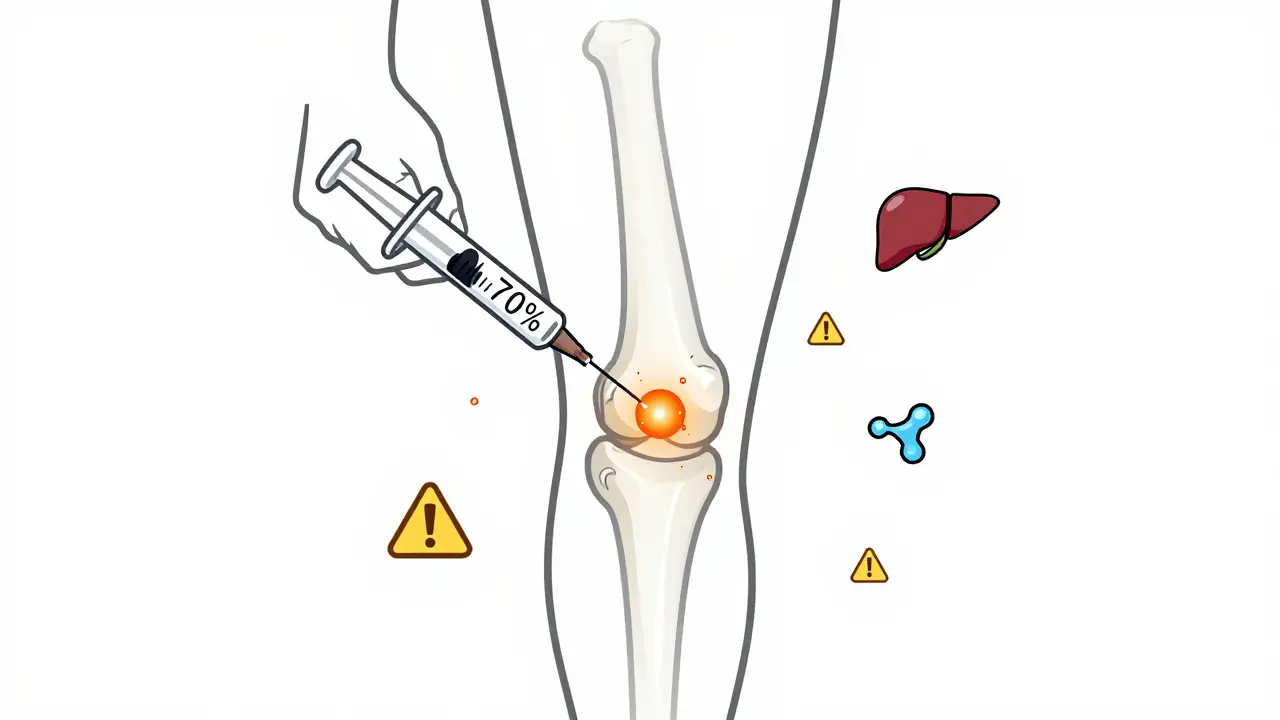
The idea behind these injections is simple: put a powerful anti-inflammatory drug - usually triamcinolone, methylprednisolone, or betamethasone - right into the joint. The goal? Reduce swelling, calm the pain, and buy some time before surgery. Doctors assume the medicine stays put. But it doesn’t. Studies show that up to 70% of the injected steroid gets absorbed into your bloodstream. Triamcinolone acetonide, one of the most commonly used forms, is especially good at leaking out. That means your liver, your adrenal glands, your bones, and your blood sugar levels all get exposed to a dose of corticosteroid - even if you never took a pill. This isn’t theoretical. In a 2023 study published in Radiology, researchers tracked patients over time and found something startling: those who got joint injections showed faster joint damage than those who didn’t. Specifically, they saw joint space narrowing by 2 mm in just 12 months - a clear sign of cartilage loss. Some even developed subchondral fractures, tiny breaks under the cartilage, or osteonecrosis, where bone tissue dies from lack of blood flow. The study found a 1% rate of these serious complications across 1,000 patients. That might sound low, but multiply that across millions of injections, and you’re talking about thousands of avoidable cases of accelerated joint failure.The Hidden Systemic Side Effects
You might think side effects are limited to a sore spot or a quick flare-up after the shot. But the real risks are systemic - they affect your whole body.- High blood sugar: Even people without diabetes can see spikes in glucose levels for days after an injection. For diabetics, this can mean emergency-level spikes that require insulin adjustments.
- Adrenal suppression: Your body makes its own cortisol - a natural steroid. When you get extra from an injection, your adrenal glands shut down. This can last for weeks. If you get sick, stressed, or have surgery during that time, your body might not respond properly. In rare cases, this leads to adrenal crisis - a life-threatening drop in cortisol.
- Bone loss: Corticosteroids interfere with bone formation and increase breakdown. This raises the risk of osteoporosis, especially in postmenopausal women and older adults. One study found that repeated injections were linked to measurable loss of bone density in the hip and spine.
- Fluid retention and high blood pressure: Steroids make your body hold onto sodium and water. This can cause swelling, weight gain, and spikes in blood pressure - dangerous for people with heart disease or kidney problems.
- Immune suppression: Even a single injection can slightly lower your immune defenses. That’s why infections at the injection site, while rare, can be serious. And if you’re on other immunosuppressants or have an ongoing infection, this increases your risk.
And here’s the kicker: these effects don’t go away after a few days. A 2018 review in PM&R found that systemic changes can linger for weeks. That means if you get a second injection four weeks later, your body hasn’t recovered from the first. Cumulative exposure matters.
How Many Is Too Many?
Most doctors tell patients to limit injections to 3 or 4 per year per joint. That’s the standard advice. But is that enough? The data says no. A 2023 analysis from the Osteoarthritis Initiative showed that patients who got repeated injections had 4.67 times higher odds of radiographic progression - meaning their joint damage showed up faster on X-rays. That number jumped from 3.2 times for one injection to nearly five times for multiple ones. And it’s not just about frequency. The dose matters. A 40 mg injection of triamcinolone isn’t twice as strong as a 20 mg one - it’s more like a 3x systemic load. When you add up all your injections - knees, shoulders, wrists - you’re not just getting localized relief. You’re building up a total steroid burden that your body can’t ignore. The American Academy of Orthopaedic Surgeons still conditionally recommends these injections for knee osteoarthritis. But their guidelines don’t account for long-term joint damage. They focus on short-term pain relief. That’s a problem.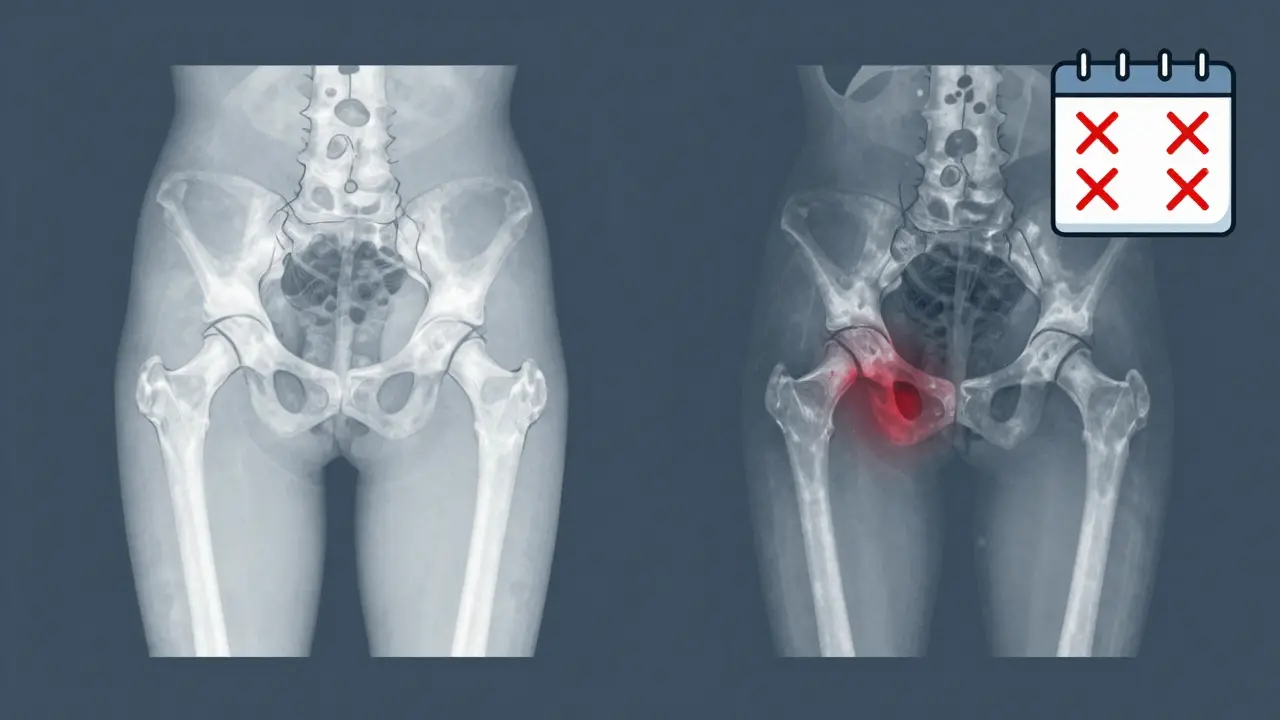
Who’s at Highest Risk?
Not everyone is equally affected. Some people are walking time bombs.- People with early osteoarthritis: If your X-ray shows only mild joint wear, but you’re in severe pain, the problem might not be arthritis at all. It could be inflammation from another source - like an autoimmune condition or even a hidden infection. Injecting steroids into a joint that’s not the real source of pain can mask the issue and let damage worsen.
- Diabetics: Even a single injection can throw blood sugar out of control. Many patients aren’t warned about this. They leave the clinic with a shot and no instructions on monitoring glucose.
- Postmenopausal women: Estrogen protects bone. After menopause, that protection fades. Steroid injections accelerate bone loss. One study found that women over 60 who got more than two injections in a year had significantly lower bone mineral density.
- People planning surgery: If you’re scheduled for a joint replacement, getting a steroid injection even 6 months before can increase your risk of infection, poor wound healing, and implant failure.
And here’s the most overlooked group: younger patients. If you’re 45 with knee pain and get an injection every few months, you might be trading short-term relief for a total knee replacement in your 50s. That’s not a trade-off most people consider.
The Controversy: Do the Benefits Still Outweigh the Risks?
There’s a reason these injections are still widely used. They work - for a while. Many patients feel better for weeks or months. For someone with severe pain and no other options, that’s huge. But the evidence is splitting. Some studies - like the one by Dr. Raynauld - found no change in joint space narrowing. Others, like Dr. McAlindon’s, showed clear cartilage loss on MRI after two years. The NIH’s 2023 debate article highlights this exact contradiction. So what do you believe? Dr. Ali Guermazi, the lead researcher on the 2023 Radiology study, put it bluntly: “We’ve been telling patients that even if these injections don’t relieve your pain, they’re not going to hurt you. But now we suspect that this is not necessarily the case.” That’s the shift happening in medicine. It’s no longer just about whether the shot helps pain. It’s about whether it’s making the disease worse. And for patients who aren’t getting better - or who are getting worse - the answer might be no.
What Should You Do?
If you’re considering an injection, here’s what you need to ask:- Is my joint damage visible on X-ray, or is the pain disproportionate to the imaging? If it’s mild or absent, think twice.
- How many injections have I had in the past year? Keep a log. Add up the total dose - don’t just count the number.
- Do I have diabetes, osteoporosis, high blood pressure, or a history of infection? If yes, the risks are higher.
- Am I planning surgery in the next 6-12 months? If yes, avoid injections entirely.
- Have I tried physical therapy, weight loss, or movement-based treatments? These are safer, long-term solutions.
And if you’ve already had injections? Don’t panic. But do get a baseline X-ray or MRI if you haven’t had one in the last year. Talk to your doctor about monitoring your bone density and blood sugar. Ask if there’s a safer alternative - like hyaluronic acid (though its effectiveness is also debated) or regenerative therapies still under study.
The Future: What’s Next?
The medical community is waking up. Researchers are now looking for biomarkers - blood tests or imaging signs - that can predict who’s at risk for joint damage from steroids. Some are testing platelet-rich plasma (PRP) and stem cell injections as alternatives. Others are developing extended-release formulations that stay in the joint longer and leak less. But until those alternatives are proven, the safest approach is simple: use these injections sparingly, only when pain is severe and other treatments have failed. And always remember - what feels like a quick fix might be a long-term cost.Can intra-articular steroid injections cause joint damage?
Yes. Multiple studies, including a 2023 study in Radiology, have shown that repeated injections can accelerate cartilage loss, lead to subchondral fractures, and cause rapid joint space narrowing. Patients with mild osteoarthritis on X-rays are at higher risk because the injection may mask worsening damage without addressing the underlying cause.
How many steroid injections are safe per year?
Most guidelines recommend no more than 3 to 4 injections per joint per year. But recent research suggests even this may be too much for some patients. The total cumulative dose matters more than the number of shots. For example, a patient who gets four 40 mg doses of triamcinolone in a year has received far more systemic steroid exposure than one who gets two 10 mg doses. Individual risk factors like age, diabetes, and bone density should guide the limit.
Do steroid injections raise blood sugar?
Yes. Even a single injection can cause blood glucose levels to rise for several days. This is especially dangerous for people with diabetes, who may need to adjust insulin or oral medications. Patients should monitor their blood sugar closely for at least 72 hours after an injection, regardless of whether they have diabetes.
Are there alternatives to steroid injections for joint pain?
Yes. Physical therapy, weight management, low-impact exercise, and nonsteroidal anti-inflammatory drugs (NSAIDs) are first-line treatments with fewer risks. Hyaluronic acid injections are sometimes used, though evidence of long-term benefit is mixed. Emerging options like platelet-rich plasma (PRP) and stem cell therapies are being studied but are not yet standard. For many, combining lifestyle changes with targeted movement can be more effective than repeated injections.
Should I avoid steroid injections if I’m planning joint surgery?
Yes. Steroid injections within 6 to 12 months before joint replacement surgery increase the risk of infection, poor wound healing, and implant failure. The immune suppression and tissue weakening caused by steroids can compromise surgical outcomes. Most orthopedic surgeons recommend avoiding these injections entirely if surgery is planned.




Dean Jones
March 3, 2026 AT 06:09Let me say this plainly: we’ve turned medicine into a vending machine. You got pain? Pop in a buck, get a steroid shot. No questions asked. But here’s the thing - your body isn’t a car with a filter you can swap out. It’s a living, breathing, hormonal nightmare that remembers every little insult you throw at it. That 40 mg of triamcinolone doesn’t just sit in your knee. It goes on a road trip - liver, adrenal glands, bone marrow, pancreas - and says, ‘Hey, we’re shutting down the natural production. Just chill.’ And when you come back for round two, three, four? Your body’s already running on fumes. The real tragedy isn’t that people get injections - it’s that they’re never told the cost. You’re not buying relief. You’re renting it. And the interest rate? Accelerated joint destruction, osteoporosis, diabetic spikes, and adrenal crashes. We’re not treating arthritis. We’re just making it look better for a few months while we quietly turn your skeleton into Swiss cheese.
Tildi Fletes
March 3, 2026 AT 17:53As a rheumatology nurse with 18 years of clinical experience, I can confirm the systemic absorption rates cited in the Radiology study are accurate. In our institution, we now track cumulative steroid exposure via a digital log - including dose, route, and timing. Patients receiving >3 injections/year show measurable drops in bone mineral density within 12 months, even when taking calcium supplements. We’ve also seen 3 cases of adrenal insufficiency requiring emergency hydrocortisone in patients who received injections within 3 weeks of viral illness. The data is not controversial - it’s underutilized. The real issue is that primary care providers, not specialists, are ordering most of these injections. Education gaps, not evidence gaps, are the problem.
Gretchen Rivas
March 5, 2026 AT 14:56My mom got 5 knee injections in 18 months. She broke her hip last year. No trauma. Just walked into a wall. Bone density scan showed T-score of -3.1. No one warned us. Now I’m the one asking the questions.
Zacharia Reda
March 5, 2026 AT 17:22Okay, but let’s be real - if you’re 68, have osteoarthritis so bad you can’t get off the couch, and PT didn’t work, are you really going to say no to 6 months of pain-free walking? The risk of joint damage is real. But so is the risk of depression, isolation, and falling because you can’t stand up. Sometimes the lesser evil is still an evil. We need better alternatives, sure. But until then, don’t shame people for choosing mobility over a theoretical future fracture. That’s not medicine - that’s moralizing.
Ivan Viktor
March 7, 2026 AT 11:18So basically, we’ve been giving people steroid bombs disguised as Band-Aids. Classic. Australia’s been limiting these to 2/year for ages. Guess what? We still have people walking. Weird.
Betsy Silverman
March 7, 2026 AT 19:56I’ve been doing physical therapy for my hip for 14 months. It’s slow. It’s frustrating. But I haven’t had a single injection. I can feel my core getting stronger. My balance is better. I’m not ‘cured,’ but I’m not deteriorating either. The idea that we need a quick fix for chronic pain is what got us here. Slow is safe. Slow is sustainable. Slow is actually healing.
Megan Nayak
March 9, 2026 AT 01:00Oh wow, another ‘the system is lying to you’ post. Let me guess - you also think vaccines cause autism and fluoride is a government mind-control tool? This isn’t medicine, it’s fear porn. 12 million injections a year? And suddenly we’re all doomed? If steroid injections were this dangerous, we’d have an epidemic of osteonecrosis in every Walmart parking lot. But we don’t. Because most people don’t get repeated injections. And those who do? They’re usually under specialist care. This article reads like a TikTok rant dressed up in PubMed citations. Chill out. Your knee isn’t about to implode.
Chris Beckman
March 10, 2026 AT 03:33bro i got 3 knee shots last year and my sugar went to 280 and i was dizzy for 3 days and my doc was like ‘oh yeah that happens’ and i was like wait what?? and then he said ‘just watch your carbs’ and that was it. no follow up. no warning. just boom. shot. go. and now i read this and i’m like oh so i was basically a lab rat. thanks doc. also i think i’m gonna get a hip shot next month. what could go wrong?
Siri Elena
March 10, 2026 AT 20:54Oh sweet summer child, you thought the steroids were just for your knee? How adorable. Did you also believe the tooth fairy pays in gold coins? Honey, that injection isn’t a magic wand - it’s a Trojan horse. Your body doesn’t care if you’re ‘just’ treating arthritis. It sees: systemic glucocorticoid assault. And your adrenal glands? They’re sobbing in the corner, whispering, ‘I used to be useful.’ You’re not ‘buying time.’ You’re mortgaging your future. And if you’re diabetic? Congrats, you’ve just upgraded from Type 2 to ‘emergency room VIP.’
Mike Dubes
March 12, 2026 AT 09:05Hey, I’m not a doctor but I’ve been reading up on this since my dad got his 4th shot last year and his bone scan looked like a Swiss cheese factory. I started doing yoga and lost 20 lbs - now my pain is 70% better. I wish someone had told us this stuff before we just kept going back. I’m not mad at the doc, I’m mad at the system. Maybe next time, ask for the data before you sign the consent form. Just a thought.