
Alopecia areata isn’t just about losing hair. It’s about waking up to a patch where your eyebrow used to be, or finding clumps of hair in your shower drain with no warning. This isn’t normal shedding. It’s an autoimmune attack - your own immune system mistakenly targeting hair follicles as if they’re foreign invaders. The result? Sudden, smooth, round bald spots, often the size of a quarter. And while it doesn’t hurt or threaten your life, the emotional toll can be crushing.
What Happens Inside the Follicle?
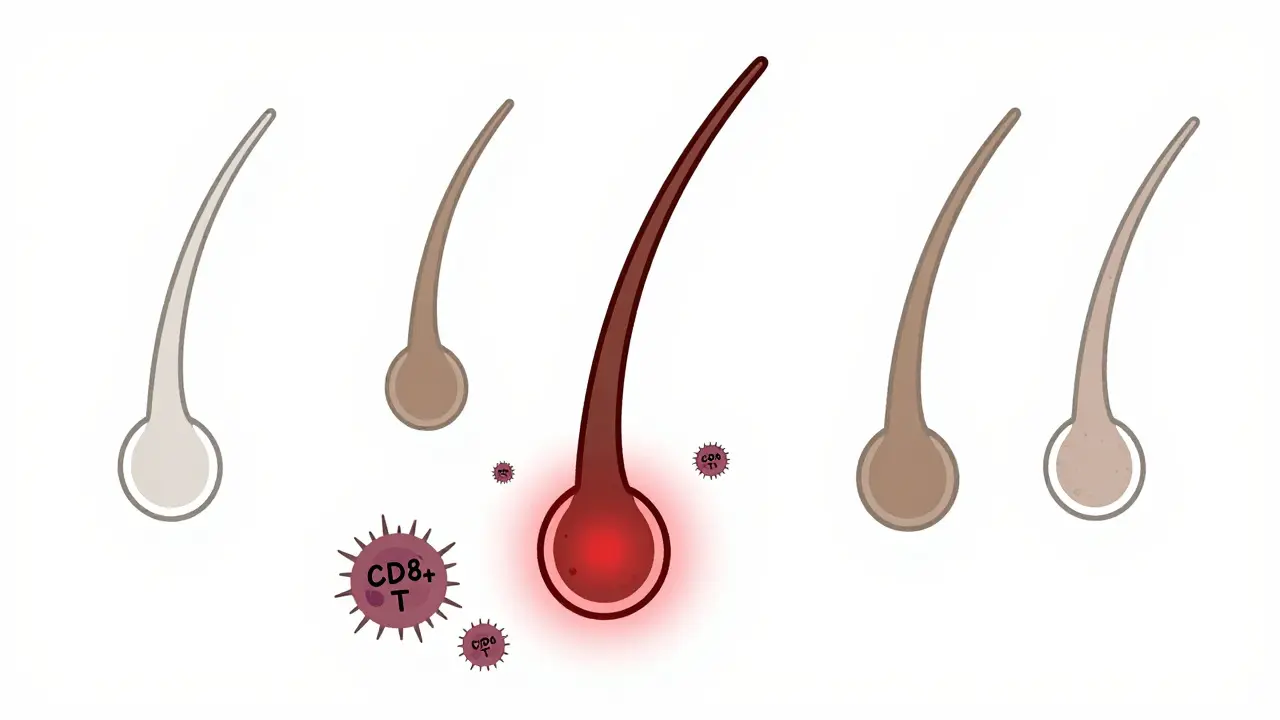
Hair grows in cycles: anagen (growth), catagen (rest), and telogen (shedding). In healthy skin, hair follicles enjoy a kind of immune shield - a "privileged" zone where immune cells aren’t supposed to interfere. In alopecia areata, that shield collapses. CD8+ T cells and natural killer (NK) cells swarm around the base of the follicle, essentially turning it off. The follicle doesn’t die. It just goes dormant. That’s why regrowth is possible - even after years of total scalp loss.Most people see one or two patches. But the condition has several forms. Alopecia areata totalis means complete scalp hair loss. Alopecia areata universalis strips every hair from your body - eyebrows, eyelashes, pubic hair, even fine body fuzz. Then there’s ophiasis, where hair loss forms a band around the sides and back of the head, and diffuse alopecia areata, which looks like sudden thinning all over - often mistaken for stress-related shedding.
Nails can betray the condition too. About 1 in 3 people with alopecia areata develop tiny pits in their fingernails, or rough, ridged surfaces. The lunula - the crescent-shaped white area at the base of the nail - may turn red. These signs aren’t just cosmetic. They’re clues that the same immune system glitch is at work.
Why This Isn’t Just "Bad Luck"
It’s not random. Genetics play a big role. Over 20 genes have been linked to alopecia areata, including ULBP3 and ULBP6 - genes involved in how immune cells recognize threats. About 20% of people with the condition have a close relative who also has it. It often shows up before age 40, and men and women are affected equally.Stress doesn’t cause alopecia areata, but it can trigger it. A major life event - job loss, divorce, illness - can push the immune system into overdrive in someone already genetically at risk. That’s why some people notice hair loss right after a traumatic event. It’s not the stress itself, but how the body responds to it.
It’s also tied to other autoimmune diseases. People with alopecia areata are more likely to have thyroid disorders like Hashimoto’s, vitiligo, or type 1 diabetes. This isn’t coincidence. It points to a deeper immune system malfunction.
How It Compares to Other Hair Loss Types
Not all hair loss is the same. Androgenetic alopecia - male or female pattern baldness - is gradual. Hair follicles shrink over time due to hormones, producing finer, shorter hairs until they stop growing altogether. There’s no inflammation. No sudden patches. Just slow thinning.Telogen effluvium is another common type. It happens after childbirth, major surgery, or crash dieting. Your body shifts hundreds of follicles into resting mode at once. You shed more than usual, but the hair grows back within 6 to 9 months once the trigger is gone.
Scarring alopecias like lichen planopilaris are different still. They destroy the follicle permanently. No regrowth possible. Alopecia areata doesn’t do that. That’s the one glimmer of hope: the follicles are still alive. They’re just silenced.
Treatment Options: What Actually Works
There’s no cure. But there are treatments - and some have changed dramatically in the last five years.Intralesional corticosteroid injections are still the most common first step. A dermatologist injects a diluted steroid - usually triamcinolone - directly into each bald patch. It calms the immune attack locally. For patchy alopecia, 60-67% of people see regrowth within 4 to 8 weeks. But it’s not magic. You need repeat injections every 4 to 6 weeks. And it doesn’t work well for total or universal hair loss. The pain is real - it stings - but results are fast.
Topical steroids - lotions or foams like betamethasone valerate - are less effective. Only 25-30% of people respond. They take 6 to 12 months. You have to apply them daily. No shortcuts. They’re better for mild cases or as maintenance after injections.
Contact immunotherapy is a more aggressive option. It uses a chemical called diphenylcyclopropenone (DPCP). You apply it weekly to your scalp. It causes a controlled allergic reaction - redness, itching, sometimes blisters. This distracts the immune system from attacking follicles. About 30-60% of patients regrow hair. But it’s messy. You need weekly visits. And the reaction can be intense. Not for everyone.
JAK inhibitors are the game-changer. These are oral pills that block the immune signals driving the attack. Baricitinib (Olumiant) got FDA approval in 2022. In clinical trials, 35.6% of patients with severe alopecia areata regrew 80% of their scalp hair in 36 weeks. Ritlecitinib, approved in June 2023, showed similar results in 24 weeks. These aren’t cosmetic fixes. They’re systemic treatments that reset the immune response.
But there’s a catch. These drugs cost $10,000 to $15,000 a month. Insurance often denies coverage. And they’re not permanent. About 75% of people lose their regrowth within a year of stopping the medication. You’re not cured. You’re managing.
The Real Cost: Mental Health and Daily Life
Alopecia areata doesn’t kill you. But it can break you.A 2022 survey by the National Alopecia Areata Foundation found 68% of patients struggled with social anxiety. 42% avoided swimming, beaches, or even going out in public. One Reddit user wrote: "I wore hats everywhere. Even in summer. I felt like I was hiding." Another said, "I cried every time I looked in the mirror. I didn’t recognize myself."
Depression and anxiety are common. Studies show 28% of patients meet the clinical criteria for depression. 30% report moderate to severe anxiety. That’s higher than the rates for psoriasis or eczema. The NIH says alopecia areata has the highest quality-of-life burden of any skin disease.
And the treatments? They add stress. Injections. Daily lotions. Waiting months for results. Financial strain from out-of-pocket costs. One patient on a forum said: "I spent $8,000 on DPCP therapy. Got no hair. Lost my job. That’s when I hit rock bottom."
What’s Next? The Road to Personalized Care
The future is promising. Researchers are mapping genetic markers to predict who will respond to which treatment. Dr. Angela Christiano’s lab at Columbia is developing a blood test that could tell you, before you start treatment, whether you’re likely to respond to JAK inhibitors. That’s huge.Combination therapies are being tested - steroids plus JAK inhibitors, or immunotherapy plus light therapy. The goal isn’t just regrowth. It’s long-term remission. The National Alopecia Areata Foundation projects a 50% reduction in disease burden by 2030.
Right now, the best approach is early action. See a dermatologist if you notice sudden patches. Don’t wait. Don’t assume it’s stress. Get tested. Know your options. And know you’re not alone. There are support groups, online communities, and new treatments coming faster than ever.
Regrowth is possible. Even after years. Even after total loss. It’s not guaranteed. But it’s real. And science is catching up.
Is alopecia areata contagious?
No, alopecia areata is not contagious. It’s an autoimmune condition, meaning your immune system attacks your own hair follicles. You can’t catch it from someone else, and you can’t spread it through touch, air, or bodily fluids.
Can stress cause alopecia areata?
Stress doesn’t cause alopecia areata, but it can trigger it in people who are genetically predisposed. Major life events - like trauma, illness, or extreme emotional pressure - can activate the immune system in a way that starts the attack on hair follicles. Managing stress won’t cure it, but it may help reduce flare-ups.
Will my hair grow back if I have alopecia areata?
Yes, regrowth is possible - even after complete hair loss. About 80% of people with patchy alopecia regrow hair within a year without treatment. For those with total or universal loss, regrowth is less common, but still happens. Hair often grows back first as fine, white or gray strands before regaining color. The follicles aren’t destroyed, just silenced.
Are JAK inhibitors safe for long-term use?
JAK inhibitors like baricitinib and ritlecitinib are FDA-approved for severe alopecia areata and have shown good safety in clinical trials. However, they carry risks like increased chance of infection, blood clots, and certain cancers. They’re typically prescribed only when other treatments fail. Regular blood tests and doctor monitoring are required. Long-term safety data beyond 2 years is still being collected.
Why do some treatments work for patchy hair loss but not total loss?
The immune attack in patchy alopecia is more localized and easier to suppress with targeted treatments like steroid injections. In total or universal hair loss, the immune response is more widespread and aggressive. Topical or localized therapies can’t reach enough follicles. Systemic treatments like JAK inhibitors are needed because they act throughout the body. That’s why corticosteroid injections have 67% efficacy for patches but only 13% for total loss.
Can children get alopecia areata?
Yes, alopecia areata often starts in childhood. About half of all cases develop before age 40, and many begin in teens or younger. Children can experience the same forms - patchy, total, or universal. Treatment options are similar but require careful dosing. Psychological support is especially important for kids, as bullying and social isolation can be severe.
Is there a cure for alopecia areata?
There is no cure yet. Current treatments manage symptoms and promote regrowth but don’t stop the underlying autoimmune dysfunction. Relapse is common, especially after stopping medication. Research is focused on finding ways to reset the immune system permanently. Scientists are hopeful that within the next decade, personalized therapies could lead to long-term remission.

Dan Mayer
March 9, 2026 AT 06:05ok so let me get this straight-autoimmune attack on hair follicles? really? i mean come on people. i read the whole thing and like 80% of this is just rewording what a med student would say in a 3rd year lecture. why are we treating this like its some new discovery? its been in dermatology textbooks since the 90s. also the jak inhibitors? yeah sure they work but did u read the side effect profile? liver toxicity, infections, lymphoma risk-this is not a spa treatment. also i saw someone say 'regrowth is possible' like its a miracle. its not. its biology. stop romanticizing it.
rafeq khlo
March 10, 2026 AT 15:52The scientific literature on alopecia areata remains profoundly underutilized in public discourse. While the article presents a surface-level overview, it neglects to contextualize the genetic polymorphisms associated with ULBP3 and ULBP6 within the broader framework of MHC class I signaling cascades. Moreover, the assertion that stress 'triggers' the condition is an oversimplification that ignores epigenetic modulation via cortisol-induced T-cell dysregulation. Clinical efficacy of JAK inhibitors must be evaluated against the FDA's black box warnings regarding venous thromboembolism and malignancy. A more rigorous analysis is warranted.
Morgan Dodgen
March 11, 2026 AT 00:46so here's the thing no one is saying lol... what if the immune system isn't 'mistakenly' attacking hair follicles? what if it's actually detecting something else? like maybe the follicles are leaking toxins from shampoos or 5G radiation or something? i mean think about it-why now? why so many cases? why do the jaks work? because they're shutting down the whole system. but what if the real problem is our environment? and they're just patching it? also i heard from a guy on a forum who said his cousin's neighbor's dog got alopecia after a wifi router was installed. coincidence? i think not 😈
Melba Miller
March 12, 2026 AT 17:12I'm sorry but this whole thing is just another way for Big Pharma to make money. You know how much I spent on that DPCP therapy? $8,000. Zero hair. Zero results. Meanwhile, the article talks about 'hope' and 'science catching up' like we're not already drowning in bills and shame. I don't need a lecture on follicles-I need someone to admit this system is broken. And stop telling me 'you're not alone.' I'm alone. And I'm tired.
Katy Shamitz
March 13, 2026 AT 04:07Oh honey, I just want to hug you all. I know how hard this is. I had patchy alopecia for 5 years. I wore scarves everywhere. I cried in the shower. But guess what? I started using a gentle scalp massage with rosemary oil and got some regrowth! Not much, but enough to feel like me again. And I found this amazing online group-everyone is so kind. You're not broken. You're just going through something hard. And you're so brave. 💖
Janelle Pearl
March 14, 2026 AT 14:27I've been living with alopecia universalis for 12 years. I didn't know anyone else who had it until I found a support group in 2019. That group saved my life. I didn't need a cure-I needed to know I wasn't a monster for looking different. I don't wear wigs anymore. I don't hide. I wear my bald head like armor. And yeah, the JAK inhibitors? I tried them. They worked for 6 months. Then I stopped. I don't want to be dependent on a $15k pill to feel like me. I am me. Even without hair. And if you're reading this and you're scared? You're not alone. Reach out. We're here.
Ray Foret Jr.
March 15, 2026 AT 09:07just got my first jaks prescription last week and already feel like a new person 😊 my eyebrows are coming back!! even the little fuzz on my arms is growing!! its like magic but real!! i know it costs a ton but my insurance covered it after i fought for it for 6 months. dont give up. its worth it. i cried when i saw the first hair. it was so tiny but it was there. i love u all 💪❤️
Samantha Fierro
March 16, 2026 AT 17:08Thank you for sharing this comprehensive overview. The clinical distinctions between alopecia areata, telogen effluvium, and scarring alopecias are critically important for accurate diagnosis and treatment planning. I particularly appreciate the inclusion of the psychosocial burden data-this is not merely a dermatological issue but a profound mental health concern that warrants multidisciplinary intervention. The emergence of JAK inhibitors represents a paradigm shift, though long-term safety monitoring remains essential. For clinicians, early referral to specialized dermatology and psychological support services should be standard of care.